

Background :
AETHERA randomized controlled study (Moskowitz, Lancet 2015) showed that the administration of Brentuximab Vedotin (BV) maintenance after autologous stem cell transplantation (ASCT) improved progression free survival (PFS) in BV-naive refractory/relapsed (R/R) Hodgkin lymphoma (HL) patients. However, since BV approval for R/R HL in 2012, many patients are receiving salvage BV before ASCT, alone or combined with chemotherapy. In the AMAHRELIS retrospective nationwide French study, we investigated the real-life outcome of patients with R/R HL mostly treated with BV-based salvage therapies and who received post-ASCT BV maintenance.
Objectives :
As primary 0objective, we assessed 2 years-PFS of patients treated with post-ASCT BV maintenance from 2012 to 2017 in France. As secondary objectives, we correlated variables (such as use of salvage BV before ASCT, centrally reviewed TEP-assessed response) with survival, and evaluated reported tolerance of BV using the CTCAE v4.0 criteria.
Methods :
We conducted this observational retrospective study in 58 national centers. Inclusion criteria were R/R HL patients who received at least two infusions of BV after ASCT, at the exclusion of patients in progression after transplant. Among 1134 patients who underwent ASCT for R/R HL between 2012 and 2017 in France based on the French society of bone marrow transplantation database, 835 (74%) patients were screened and data were available for 794 (70%) patients. FDG-PET scan at relapse and before transplantation were recorded and centrally reviewed (still ongoing). FDG-PET scan were reported using the Deauville score (DS), and complete remission was defined by a DS < 4. Post-transplant status was evaluated based on CT-scan or on FDG-PET scan results. This study was approved by the SFGMTC and the LYSA.
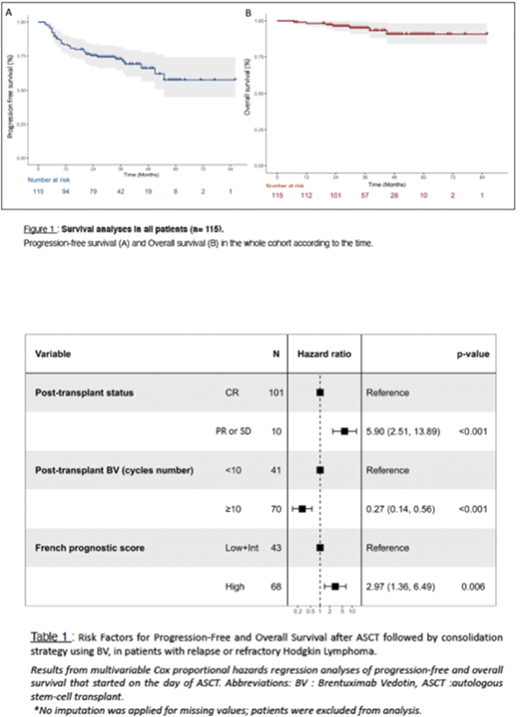
Results : Fifteen percent (115/794) of patients met eligibility criteria, and were enrolled in this study. Among them, 95% met inclusion criteria for BV maintenance according to the AETHERA study as primary refractory disease (43%), early relapse (27%) or extranodal disease (49%). The mean number of BV injections after ASCT was 11 (3-18). Patients characteristics were : mean age was 34 y (range between 16-70y), 54% were male, and 57% of patients were stage III or IV at relapse. Notably, 70% of patients received BV as salvage therapy and 81% achieved a complete remission before ASCT. The median follow-up period was 35 months. The 2 years survival for the whole cohort was 75,3% for PFS (95% CI : 68,4-84,3) and 96,4% for overall survival (95% CI : 94,2-100) (Figure 1). The use of BV as part of salvage therapy before transplant had no impact on PFS. We observed a trend to an increased occurrence of neuropathy in patients receiving BV before transplant without impact on early treatment discontinuation. We tested several variables for correlation with survival using a univariate Cox model including high risk patients defined as primary refractory disease or early relapse and disseminated disease, extranodal relapse, use of BV before transplant, number of salvage lines, remission status before and after transplant (complete response versus partial response or stable disease), time between ASCT and BV onset and number of BV cycles after transplant. Among these variables, high risk status, less than 10 post transplant BV cycles and absence of post transplant complete remission significantly correlated with a reduced survival probability, and remained significant after analysis using a multivariate Cox model (Table 1).
Conclusion :
From the real-life AMAHRELIS study, we confirmed the very good outcome of R/R HL patients in the era of post-transplant BV maintenance, with a 2y-PFS of 75% similar to the results of the AETHERA landmark study (2y-PFS of 63%). The results of current strategies with pre- and post-transplant BV outperformed historical series based on high dose therapies, including those of tandem transplant for high risk patients. Future studies incorporating BV strategies with immune checkpoint inhibitors might improve outcome in R/R HL patients.
Meignan:ROCHE: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company). Sibon:takeda france: Consultancy. Stamatoulas Bastard:Pfizer: Other: TRAVEL, ACCOMMODATIONS, EXPENSES; Celgene: Honoraria; Takeda: Consultancy. Fornecker:Takeda: Consultancy; Roche: Consultancy. Casasnovas:Takeda: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company), Research Funding; Roche: Consultancy, Honoraria, Other: travel, accomodations, expenses, Research Funding; Gilead: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company), Research Funding; Abbvie: Consultancy, Honoraria; MSD: Consultancy, Honoraria; Amgen: Consultancy, Honoraria. Cartron:Gilead: Honoraria; Jansen: Honoraria; Abbvie: Honoraria; Celgene: Consultancy, Honoraria; Sanofi: Honoraria; F. Hoffmann-La Roche: Consultancy, Honoraria. Ghesquieres:Gilead: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES; CELGENE: Consultancy, Other: TRAVEL, ACCOMMODATIONS, EXPENSES; Roche: Consultancy, Other: TRAVEL, ACCOMMODATIONS, EXPENSES; Janssen: Honoraria. Brice:Takeda: Consultancy; Roche: Consultancy. Hermine:AB Science: Consultancy, Current equity holder in publicly-traded company, Honoraria, Patents & Royalties, Research Funding; Celgene BMS: Consultancy, Research Funding; Roche: Consultancy; Novartis: Research Funding; Alexion: Research Funding. Rubio:Medac: Consultancy; Gilead: Honoraria; MSD: Honoraria; Novartis: Honoraria; Neovii: Research Funding. Deau Fischer:Takeda: Consultancy; Roche: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal